
Why Plasmapheresis?
Introduction
Perfusionists use sophisticated technology to effectively manage a patient's blood during cardiopulmonary bypass.
Terumo Cardiovascular Systems is committed to providing customers with products that advance their blood management goals. Just as Terumo's Prescriptive Oxygenation™ approach helps clinicians reduce prime volume and hemodilution, Terumo also distributes a device used in cell salvaging and plasmapheresis that can help limit the need for allogeneic blood. This article is the second in a series of articles that focuses on the unique technologies that Terumo offers.
 History of Plasmapheresis
History of Plasmapheresis
Platelet dysfunction is a significant factor in postoperative bleeding following cardiopulmonary bypass (CPB) and other surgical procedures with high blood loss. Clinicians rely on plasmapheresis to reduce post-operative bleeding or coagulopathy, and the need for allogeneic blood transfusions, by returning functional platelets and coagulation factors to the patient.
Plasmapheresis was first used therapeutically in the early twentieth century, but it wasn't until after the 1940s that the practice was adopted on a larger scale. Today's plasmapheresis devices — both "blood bank" systems and "cell salvagers" — rely on centrifugation to separate blood's constituent elements. Of note, all of these centrifugal systems owe their origins to a continuous flow centrifuge developed for the dairy industry in 1878 that separated cream from milk.
An Overview of Plasmapheresis
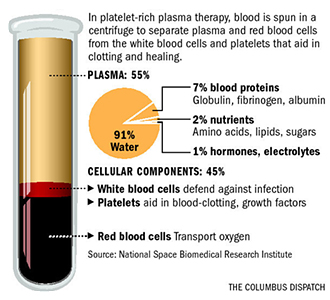
Working with anesthesiology, the perfusionist initiates plasmapheresis after anesthetic induction but before CPB. Drawing from the side-port of a Swan-Ganz introducer, the patient's blood is diverted into a centrifuge-based device where the platelet rich plasma (PRP) is separated from the red blood cells (RBC) and platelet poor plasma (PPP). The RBCs can be returned immediately to the patient, while the PRP is transferred to a bag containing citrate and administered at the completion of bypass (or at the end of the procedure in orthopedic cases with high blood loss).
 Continuous high speed centrifugation produces a PPP product, but fast centrifugation followed by slow centrifugation sequesters more platelets and returns both platelet rich and platelet poor plasma.
Continuous high speed centrifugation produces a PPP product, but fast centrifugation followed by slow centrifugation sequesters more platelets and returns both platelet rich and platelet poor plasma.
Platelets, or thrombocytes, are cytoplasmic, non-nucleated cell fragments derived from bone marrow megakaryocytes. A healthy human typically has between 180,000 and 400,000 platelets in their body.
Activated platelets are critical to wound healing and angiogenesis by releasing growth factors and chemotactic factors. Regardless of the substance or material that triggers the reaction, activated platelets demonstrate the same series of responses: change in shape (from a disc to a spiny sphere), aggregation, secretory events, and the release of arachidonic acid. Clinicians take extreme care to prevent premature platelet activation. Because platelet activation can occur when blood is exposed to the non-biological extracorporeal circuit, plasmapheresis plays a key role in sequestering the patient's platelets and coagulation factors without exposing them to the perfusion circuit, thus preventing the risk of platelet activation and diluted coagulation factors.
Clinical Evidence for Plasmapheresis
For many years, the theoretical value of plasmapheresis was not supported by the totality of clinical evidence. However, more recent studies have confirmed the merit of platelet sequestration under specific conditions. In fact, the 2011 update to the STS blood conservation guidelines recognized the value of plasmapheresis:
|
An earlier meta-analysis of 20 plasmapheresis studies found that the "use of platelet-rich plasmapheresis results in improved clinical outcomes for patients when compared to those on whom PRP is not used. These improved clinical outcomes result in 25.4% lower costs per patient on whom platelet-rich plasmapheresis is used."
In another study presented at the 20th Annual Symposium on New Advances in Blood Management, Duke University Hospital researchers compared 24 apheresis procedures (using the TerumoBCT Trima Accel® Automated Blood Collection System) with 24 similar but non-apheresis procedures. They found that only 29% of patients in the apheresis group received allogeneic platelets, while 83% of patients in the non-apheresis group received allogeneic platelets.
To achieve optimal hemostasis, the STS guidelines recommend harvesting at least 3 x 1011 platelets, or 28% of the patient's circulating platelet volume.
Fresenius C.A.T.S®plus Autotransfusion System
By using the disposable plasma sequestration (PSQ) set in conjunction with the standard AT1 set, clinicians can practice plasmapheresis and cell salvage in a single device. Performed pre-operatively, the PSQ program consists of four stages:
-
 Plasma sequestration: During this phase, the shed blood is separated under centrifugal force. The packed red cells are delivered into the PRC or reinfusion bag which also transfers air and plasma into the plasma bag. The buffy coat, comprised of platelets and white blood cells, is enriched in the washing chamber during this phase.
Plasma sequestration: During this phase, the shed blood is separated under centrifugal force. The packed red cells are delivered into the PRC or reinfusion bag which also transfers air and plasma into the plasma bag. The buffy coat, comprised of platelets and white blood cells, is enriched in the washing chamber during this phase. - PRC transfer: During the PRC transfer stage, the residual RBC volume is delivered from the washing chamber into the PRC bag. To replace the volume withdrawn from the washing chamber, plasma flows via the saline pump into the washing chamber. This phase concludes automatically when the residual RBC volume is completely delivered into the PRC bag.
- PRP transfer: During the third phase, PRP is transferred from the washing chamber into the PRP bag. Once 100mL of PRP have been delivered into the PRP bag, this phase ends and the final plasma transfer phase begins.
- Plasma transfer: In the final phase, the residual plasma volume from the washing chamber is transferred into the plasma or PRC bag.
Using the C.A.T.S®plus device on 500mL of shed blood with a baseline hematocrit of ~34% and a baseline platelet count of ~189,000/mL, the typical platelet yields in the PRP product are:
- Average PRP volume: 89mL
- Average platelet count: 605,000/mL
- Average platelet yield: 0.54 x 1011
- Average platelet recovery rate
- 51% in PRP product
- 21% in plasma product
The average processing time for 500mL of whole blood is eight minutes. To achieve the platelet yield recommended by the STS, clinicians should complete five or six "passes" each, for a total of 40-50 minutes of processing time.
Conclusion
Terumo offers clinicians advanced technologies that allow them to make informed decisions about patient care with the products they choose. The innovation behind the Fresenius C.A.T.S®plus system makes it an important component of any blood management program. As the U.S. distributor for the C.A.T.S®plus device and a recognized leader in innovation, Terumo was ranked 14th on Forbes Magazine's list of the World's Most Innovative Companies. Future issues of "Quarterly Updates in Optimizing Cardiac Surgery" will continue to highlight the unique and innovative technologies at the heart of Terumo's portfolio of products.
References
Boldt, J, et al. (1993). Influence of acute preoperative plasmapheresis on platelet function in cardiac surgery. J Cardiothorac Vasc Anesth.
Counts, R. (1998). Chapter 6: Physiology of Hemostasis. Perioperative Transfusion Medicine. Williams & Wilkins.
Ereth, M, et al. (1998). Chapter 22: Intraoperative Techniques to Conserve Autologous Blood: Red-Cell Salvage, Platelet-Rich Plasma, and Acute Normovolemic Hemodilution. Perioperative Transfusion Medicine. Williams & Wilkins.
Ferraris, V, et al. (2011). 2011 Update to The Society of Thoracic Surgeons and the Society of Cardiovascular Anesthesiologists Blood Conservation Clinical Practice Guidelines. Ann Thorac Surg.
Fresenius C.A.T.S®plus Autotransfusion System Operating Instructions.
Fresenius C.A.T.S®plus More than saving cells CD-ROM.
Mahoney, C. (1998). Platelet-Rich Plasmapheresis: A Meta-Analysis of Clinical Outcomes and Costs. JECT.
Slichter, S. (1998). Chapter 5: Platelet Production, Physiology, Hemostasis, and Transfusion Therapy. Perioperative Transfusion Medicine. Williams & Wilkins.