
A Comparative Study of Endoscopic Vein Harvesting Systems
In his presentation at Terumo's Optimizing Conduit Quality workshop at the Annual Meeting of the Association of Physician Assistants in Cardiovascular Surgery (APACVS) in January 2010, Jeffrey D'Agostino, M.S., PA-C, opened the discussion of his study of comparative EVH systems with a question: traditional open technique vein harvesting is well proven, rapid, provides optimal visualization of the vein during harvesting and is cost effective, but is it good for the patient?
Background: For many patients, coronary artery bypass graft (CABG) surgery is the only definitive means for treating coronary artery disease.1 The goal of CABG surgery is to increase perfusion to ischemic myocardial cells distal to the obstructed portion of the coronary artery. Increasing the blood flow to the distal portions of the heart is achieved with bypass grafts, or conduits, that are attached below the narrowed portion of the artery. Commonly used conduits in CABG surgery are the internal mammary arteries, radial arteries, and the greater saphenous vein. Despite the recent trend of using arterial conduits for coronary revascularization, the saphenous vein remains an essential and the most commonly-used conduit for CABG procedures because it can be tailored to various lengths to fit anywhere across the heart.
The success of CABG surgery is dependent on the quality of the conduit selected, primarily its long-term patency.3,4 Long-term patency of a bypass graft is an important determinant in reducing morbidity and increasing survival after coronary bypass surgery. Graft failure has consequences similar to those of coronary artery disease, including recurrent angina, myocardial infarction (MI), additional revascularization procedures, and premature death. Obtaining a high quality graft and maintaining its endothelial integrity are two critical components of successful surgery, an uneventful postoperative course, and improved long-term survival.
Endoscopic vein harvesting (EVH) is the standard of care for patients who require saphenous vein grafts for coronary and lower limb revascularizations.5 Today, EVH has become the procedure of choice in harvesting saphenous veins for CABG procedures; approximately 80% of cardiac surgery centers offer EVH as a modality for saphenous vein harvesting.6
Study Reveals Differences in Thermal Spread and Branch Length
Although several EVH systems are commercially available, few studies compare the merits and demerits of each system. Through a small case study, Terumo aimed to bridge the gap that exists in available literature.
Three metro New York hospitals agreed to participate in a case study that involved 48 EVH cases. St. Barnabas Healthcare System, NJ contributed 64.58% of the cases while Staten Island University Hospital, NY and Montefiore Medical Center, NY contributed 18.75% and 16.67% of the cases respectively.
The two EVH systems under review were the VirtuoSaph® Endoscopic Vein Harvesting System from Terumo and VasoView® 7xB System from Maquet Cardiovascular.
Objectives and Hypothesis of the Study
The first objective was to determine the extent of thermal injury, if any, to the harvested vein. The second was to verify vein branch length. The hypothesis was that:
- VirtuoSaph System would have less thermal spread due to its simultaneous coagulation-cut energy delivery.
- Use of the VirtuoSaph System would provide longer branches as a result of the mechanical design of the V-cutter that has a fixed distance between it and the vein keeper (V-keeper). The requirement to ground to the tunnel wall during coagulation and cutting was another contributing factor in branch length.
Methodology
- Thermal Spread: Rated per clinician judgment. Marked as "yes" or "no".
- Branch Length: Each branch was measured with a ruler or equivalent measuring device. A picture was taken to show that branch length was not manipulated to achieve length measurement.
- 'Convert to open vessel harvesting' was reported.
*For both systems, cautery was set between 18-25 watts. CO2 was infused at a rate of 3-5 L/min to a pressure of 10-15 mmHg. Patients that were excluded were those who had COPD, peripheral vascular disease, chronic administration of steroids, end stage renal disease receiving hemodialysis, or who were 85 years and older. Inclusion criteria were any patient requiring CABG per the participating institution's diagnosis who did not fall into the exclusion criteria.
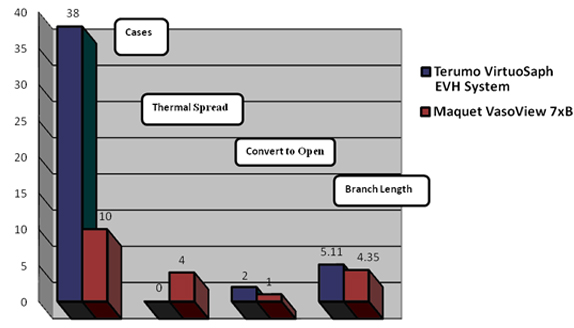
Results
- A total of 48 cases were recorded. Thirty-eight using VirtuoSaph EVH System and 10 using VasoView 7xB. (N=48)
- Eight percent of the total cases showed macroscopic thermal damage. Zero percent of the VirtuoSaph EVH System cases resulted in thermal damage while 40% of VasoView 7xB cases resulted in thermal damage.
- Average branch length for VirtuoSaph EVH System cases was 5.11 mm and 4.35 mm for VasoView 7xB.
- Six percent of the total cases resulted in convert to open. Five percent of the total VirtuoSaph EVH System cases were converted to open. Ten percent of the total VasoView 7xB cases were converted to open.
Conclusion
Thermal spread was lower and branch length longer using the VirtuoSaph EVH System in comparison with the VasoView 7xB system.
Despite a perceived compromise in equality of the operative procedure results, EVH remains a minimally invasive procedure that causes a decrease in patient morbidity. The results of this study are more appropriately used as preliminary data to support the design of a randomized trial that will provide more definitive conclusions in these areas.
1 Anstadt MP, Franga DL, Portik-Dobos V, Pennathur A, Bannan M, Mawulawde K, Ergul A. Native matrix metalloproteinase characteristics may influence early stenosis of venous versus arterial coronary artery bypass grafting conduits. Chest. 2004; 125(5): 1853-1858.
2 Seifert PC, Collins J. Cardiac surgery. Competency for Safe Patient Care During Operative and Invasive Procedures. Denver, CO: CCI; 2009: 720.
3 Buxton BF, Hayward PAR, Newcomb AE, Moten S, Seevanayagam S, Gordon I. Choice of conduits for coronary artery bypass grafting: craft or science? European Journal of Cardiothoracic Surgery. 2009;35:658-670.
4 Vein Graft Failure in Coronary Artery Bypass Surgery. Available at: http://medicineworld.org/cancer/lead/11-2005/vein-graft-failure-in-coronary-artery-bypass-surgery.html. Accessed February 5, 2010
5 Allen KB, et al. Endoscopic vascular harvest in coronary bypass grafting surgery: a consensus statement of the ISMICS, Innovations 1 (2005), pp. 51-60
6 Braxton JH, Ryan C, Christie A, Kane J, Kramer RS. Intraoperative angioscopy for endoscopic veins: a simple quality control measure. Available at: http://www.ctsnet.org/sections/clinicalresources/videos/vg2009_KramerR_intraopAngioscopy.html. Accessed February 5, 2010
About Jeffrey D'Agostino, M.S., PA-C

Jeffrey D'Agostino, M.S., PA-C, is board certified by the National Commission on Certification of Physician Assistants (NCCPA). He is licensed and registered with the State of New Jersey. A graduate of Seton Hall University of Medicine and Dentistry in Newark, New Jersey with a Master of Science - Physician Assistant degree, he holds a Bachelor of Science degree magna cum laude in Molecular Biology from Montclair State University in Montclair, New Jersey. Mr. D'Agostino is a member of the Association of Physician Assistants in Cardiovascular Surgery. He is a resident of Teaneck, New Jersey.
Prior to his appointment as Chief Physician Assistant at the St. Barnabas Heart Centers located in Livingston and Newark, New Jersey, he served as a physician assistant in cardiothoracic surgery for over eight years. He takes great satisfaction in working in both the operating room and patient units to contribute his skills and energy to making patient outcomes the best they can possibly be.
About The Heart Center at Newark Beth Israel Medical Center
Newark Beth Israel Medical Center, an affiliate of the St. Barnabas Health Care System, was named among the nation's top 50 hospitals for specialty care in Heart and Heart Surgery by U.S. News Media Group's 2009-10 America's Best Hospitals. Now in its 20th year, America's Best Hospitals guide ranks hospitals that excel in specified kinds of medical and surgical care based on a variety of rigorous criteria.

